Reviewed by Stacey Gunn, MD.
Research by Savit Malhotra and Quynh Theresa Do.
Introduction
Over the past month, our “Crash Course” has extensively discussed the dopaminergic mechanism and various treatments to manage the symptoms of Restless Legs Syndrome (RLS). For the next two weeks, our focus will be shifted to iron and its mechanism in RLS. As highlighted by Harvard Health, addressing iron deficiency has been recognized as a “simple treatment” that can significantly relieve RLS symptoms due to iron’s involvement in the neurological systems impacted by the condition.[1] But how do iron supplements work at a cellular and systems level to mitigate RLS symptoms? In this week’s article, we will review iron’s role, its metabolism, and, specifically, its mechanism within the pathophysiology of RLS.
Iron’s Role in Brain Function and Dopamine Production
Iron is an essential micronutrient responsible for numerous physiological processes across every system in the body. Its most widely known function involves the circulatory system. The vast majority of iron in the human body is used by the bone marrow to create hemoglobin in red blood cells, which are responsible for transporting oxygen from the lungs to peripheral tissues.[2] However, iron’s role in the brain and central nervous system is critical for conditions like RLS. In the brain, iron acts as a helper molecule (scientifically known as a cofactor) for proteins known as enzymes to jump start (or catalyze) certain biochemical processes. These include energy production processes (e.g., cellular respiration) and the synthesis of neurotransmitters.[3]
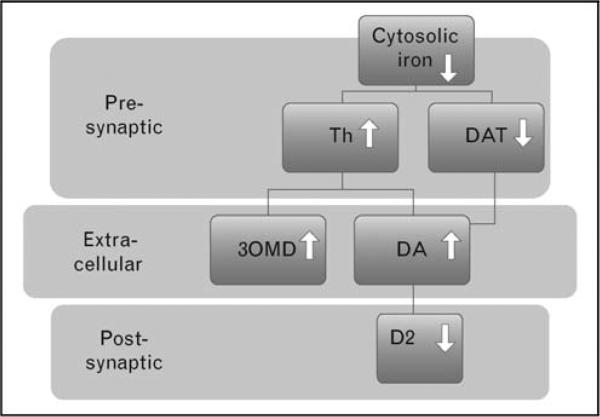
Among the processes, iron has a function in the dopaminergic pathway, which has been mentioned in a previous blog post. Iron deficiency has been tied to worsening symptoms of RLS through the dopaminergic pathway.[4] However, the relationship between iron deficiency and dopamine in RLS is more complex than simply "low iron equals low dopamine." Iron is an essential catalytic metal center of tyrosine hydroxylase (Th), an enzyme that converts the amino acid L-tyrosine into L-dopa (levodopa), which is then converted into dopamine. Interestingly, brain iron deficiency in RLS appears to create a paradoxical increase in dopaminergic activity.[5] As a result, certain brain regions, particularly the striatum, can go into a hyperdopaminergic state.[6]
The effect above happens even though blood iron levels may be completely normal. The problem lies in how iron gets into the brain through the blood-brain barrier. Brain iron deficiency disrupts iron homeostasis at the blood-brain barrier level.[7] This is particularly seen in the brain regions of the substantia nigra and the striatum, both areas of the brain vital to dopamine production.[5] The resulting disruption in dopamine signaling within the motor and sensory circuits is thought to contribute significantly to the uncomfortable sensations and urge to move experienced by individuals with RLS.[8,9] Correcting this iron deficiency is thus a primary therapeutic target to alleviate RLS symptoms.
The Role of Oral Iron Supplementation in RLS
When it comes to RLS, iron plays a central role in the pathophysiology due to its involvement in dopamine production. Iron aids the enzyme tyrosine hydroxylase, which regulates the production rate of dopamine.[10] It is believed that when the pathway to produce dopamine is disrupted, the characteristic sensory and motor symptoms of RLS may present.[11] Interestingly, numerous studies have found that individuals suffering from RLS often have reduced iron levels within the brain, particularly in the the basal ganglia (where dopamine production pathways occur).[10,13] Therefore, scientists hypothesize that iron deficiency is likely one cause for RLS, which leads us to iron supplementation as a potential treatment. However, it is important to note that those with reduced iron levels may still exhibit normal blood iron levels due to iron not being transported across the blood-brain barrier (there are very few ways in which substances can cross the blood-brain barrier).[10,13,14] Therefore, those with “normal” blood iron levels may still benefit from iron supplements.
To evaluate iron status, clinicians typically rely on an iron panel that includes serum ferritin, serum iron, transferrin, total iron-binding capacity (TIBC), and transferrin saturation (TSAT).[15] Of these, serum ferritin tends to be the most useful marker due to it reflecting long-term total body iron stores (whereas iron levels can fluctuate day to day, or even throughout the day), followed by TSAT, which increases with oral iron supplementation (there are two primary ways in which iron supplements can be administered: orally (via a tablet or pill) or intravenously (IV, which we will focus more on next week). While IV methods of administration often works faster with fewer gastrointestinal side effects, oral iron supplements still have their place).[16,17] However, TIBC tends to decrease as iron availability improves.[16]
Compared with other RLS treatments that we have discussed, oral iron supplements remain a practical and accessible early treatment option. Typically, iron is prescribed as ferrous sulfate 325 mg, which corresponds to approximately 65 mg of elemental iron (the active component responsible for replenishing iron stores).[18] Previously, some guidelines advised taking multiple doses per day, but this is no longer the case. Recent studies have found that less frequency dosing make actually improve absorption.[19] This is because oral iron intake increases hepcidin levels, a regulatory hormone that reduces intestinal iron absorption for up to 24-48 hours after ease dose. Therefore, the current guidelines recommend once-daily or every-other-day dosing, which has been shown to enhance absorption while also minimizing side effects (such as nausea).[19]

One important note is that in some cases, oral iron supplements may not be the best option and instead, IV iron should be given. For patients with a serum ferritin level <75 ng/mL, oral iron (typically 325-650 mg ferrous sulfate daily or every other day) or IV iron are both reasonable options.[20] However, when ferritin levels fall between 75-100 ng/mL, oral iron becomes less effective due to reduced absorption, and IV iron is generally preferred.[21] In patients with ferritin levels above 100 ng/mL but below 300 ng/mL, some data suggest that IV iron may still provide benefit, though this approach extends beyond standard guideline recommendations.[22] Finally, iron supplementation should be avoided in individuals with >300 ng/mL or transferrin saturation >45%, as excess iron can increase the risk of hepatic iron overload.[23]
However, we want to emphasize that this dose may not be the right dosage for you. Other factors (such as the health of your liver, past medical history, and other medications/supplements) should be taken into account when dosing ferrous sulfate. For this reason, we recommend that you see a medical professional before beginning to take ferrous sulfate, and keeping in regular contact with them while you treat your RLS. Ferrous sulfate also works best on an empty stomach or when taken with vitamin C (some hypothesize that both increase absorption of the supplement).[24] Those who are taking ferrous sulfate should also avoid consuming dairy products within 2 hours before or after taking ferrous sulfate. This is because dairy products can actually inhibit absorption.[25] Clinical evaluations have found that oral iron supplements are most effective in patients with lower ferritin levels and mild-to-moderate RLS symptoms.[16,26]
Those who are taking iron supplements should know that the effects are not immediate. Typically, those taking ferrous sulfate may begin to see improvements in their symptoms after 4 to 8 weeks, with maximal effects often taking 1 to 3 months or longer.[26] Patience is key when it comes to treating chronic diseases, and we would encourage you to consider all options and give each ample time to take effect before moving on to the next treatment.
Conclusion
Of all of the treatment options that we have seen, iron supplements tends to be among the safer and more frequently recommended. The current treatment guidelines list ferrous sulfate as being a conditional recommendation with moderate certainty of evidence, while IV iron infusions have a stronger recommendation (which we will discuss more in our next article).[17] However, treatment is never “one size fits all.” What works for one person may not work for another and, similarly, what doesn’t work for one may work for another. For this reason, we recommend that before you begin treating your RLS, you seek out the advice and help of a professional. The team here at Empower Sleep is always ready to assist you!